
Coding Best Practices for Ketamine Clinics
Most outpatient out-of-network services like a visit to a doctor or therapist utilize fairly simple medical coding–there’s usually just one (or maybe two) service codes (also known as CPT, or Current Procedural Terminology codes). But as new treatments go out-of-network, like ketamine infusions for depression, medical coding needs to adapt.
The Basics: Inpatient vs. Outpatient coding
Inpatient vs. outpatient coding can be miles apart. This major difference has been caused by the tortuous history of hospital reimbursements from insurers, which make up as much as 97% of hospital payments.
At in-network hospitals, the more procedures and codes that are on the bill, the higher their payment.
From: How did hospital bills get so complicated?
by Lisa Zamosky, LA Times
Insurers have been pushing for decades to move more services from inpatient to outpatient in an effort to reduce costs and therefore the reimbursement dynamics are different.
IN-network vs. OUT-of-network coding
Due to cost-containment pressure driving individual CPT code reimbursements down, there has been a tendency by practitioners and hospitals to code for every service code that is allowed, like an E&M (evaluation and management) service, an EKG (echocardiogram), or perhaps a blood draw. The biller knows that the EKG and blood draw might only get reimbursed a few dollars or, in some cases, nothing at all. But there’s really no downside to this strategy since the rendering provider “accepts assignment” — a fancy way of saying, “despite what my billing amounts are, I agree to accept what our contract says.” Reimbursements are not typically slowed down.
However, since there is no contract between an out-of-network practitioner and an insurer, the out-of-network service billed this way might cause the entire claim to be flagged and await involvement by the practitioner or patient to clarify the issues. This is in addition to the fact that there seems to be more scrutiny applied to out-of-network bills in general. Result: OON reimbursements are slowed down.
Below you will find some generalized guidance — but remember, practitioners should seek opinions from their own billing/legal experts on the optimal and appropriate coding strategy for their practices.
Superbill Coding Tips to Ensure Accuracy (and Reimbursability) for Ketamine Infusion Services
Infusion Codes (96365 and others)
These are the most common codes for ketamine infusions (big surprise!). The CPT code 96365 is used for infusions up to 90 minutes in duration.
A full list of infusion and injection codes can be found on the American Academy of Professional Coders (AAPC) website here: Infusion & Injection Coding – AAPC
This is a high-yield, low-friction billing strategy.
Evaluation (E&M) Codes (99201-99205)
These are perfect for your initial assessment of a patient on a visit for which an infusion was NOT given.
If an infusion occurred, it usually takes precedent–an E&M code should not be billed on the same day.
Exception: An E&M code CAN be billed if a new or separate clinical issue was evaluated. In this circumstance, the E&M code would be billed with the modifier “25”
When appropriate, this is a high-yield, low friction billing strategy.
Vital Signs and EKGs (e.g., 99211)
If an infusion or E&M service was billed for that date of service, then the vital signs are bundled into that service, even if the vitals were checked by someone other than the primary practitioner
If the patient only came in for a check of vital signs (done by someone who is not independently licensed), then the code of 99211 can be used.
This is a low-yield, high friction billing strategy.
EKGs (93000, 93005, 93010)
Again, standard EKGs as part of infusion or E&M services would not be billed separately.
In addition, this is usually a low-priced service (Medicare reimbursement averages < $20), so including this code for OON services is a high-risk, low-reward strategy
If an EKG needs to be billed, however, it can be done if it is due to a new/separate complaint, they can be billed with the modifier “59” alongside an infusion or E&M service.
This is a low-yield, high-friction billing strategy.
And what about J-codes?
No self-respecting hospital biller would fail to include billing for “J” codes for the actual medication given during an infusion. It’s just what is right. The pharmacy department at a clinic or facility is likely run as an independent business and has to cover its own costs. In addition, due to the downward pressure on reimbursements, it might not be feasible to “absorb” medication costs into the fees for other services.
However, for out-of-network services involving relatively inexpensive medications (<$50 per dose or infusion), it’s likely best to exclude the J codes from the superbill. Why? Some medications, like lidocaine, are assumed to be bundled into the infusion or E&M service. In addition, for J-codes to be successfully billed, most insurers require NDC codes for the medication used as well as dosage and method of administration.
This is a low-yield, high friction billing strategy.
Finally, let’s look at two different methods of coding for the same infusion appointment:
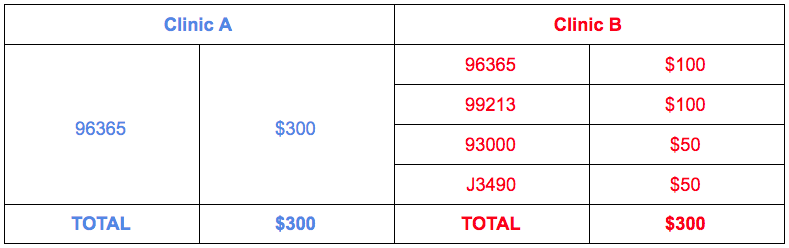
Data from Reimbursify claims history shows that patients see an easier and higher level of reimbursement for OON services from Clinic A than from Clinic B, when all else is equal.
We hope this has been helpful! Again, please consult a professional coder for specific guidance for your practice.
Note: Any coding guidance provided by Reimbursify has been vetted through our Certified Professional Coders and/or health care attorney consultation but this does not substitute for obtaining your own coding consultation with a specialist.
Contact us today to learn more!